


Support Groups For Parents of Trans Kids Are Echo Chambers


Before anything else, a disclaimer: I am not, and do not claim to be any kind of expert in transgender healthcare for kids. I am just a parent trying to get an honest understanding, enough to be able to advise my child. I am asking questions and trying to learn. I am looking for answers – I’m not under the misapprehension I already have all of them.
I don’t think it is radical to say that it is a parent’s responsibility, above all else, to keep their child safe. I think most parents feel as my wife and I do: that we would throw ourselves under the proverbial bus if it was ever necessary and, certainly, when a difficult situation arises, we will gladly take on any part of the burden if it spares our child pain.
If we are going to fulfil that duty, we have to be willing to ask difficult questions, even if it is uncomfortable or unpopular. It’s not our job to make our own lives easy, it’s our job to leave no stone unturned when it comes to safeguarding our children.
However, I was thrown out of a group that is supposed to support parents of transgender kids recently, for doing exactly that. I wanted to have a discussion about the safety of potential treatments, and the evidence that supports it. Apparently, wanting to do this is transphobic.
You may be thinking “there must be more to it than that” and, of course, there is. But, ultimately, the line appears to be drawn that it is more important not to upset or worry those parents who might not like to be challenged than it is to try to help parents get to the actual truth regarding the safety of their kids.
I have found this in more than one place that was marketed as being there to support me as the parent of a transgender child, and I have yet to find anywhere at all I can have a reasonable, evidence-based discussion about this without it descending into accusations of transphobia.
I wouldn’t blame you for thinking I must have done something horrible. It sounds awful to be accused of being transphobic. I must be a hateful monster. And perhaps I am, and I am simply too stupid or bigoted to be able to see it. You can judge for yourself.
There is quite a lot of context here but please bear with me - I think it is all important. I’ve tried hard to keep it as concise as I can, but I also don’t want to make assumptions about what people know, nor do I want to skip over my own reasoning. I’ve included conversations I have had, but have hidden the names, to protect privacy – I do not want to be the cause of any pile-ons.

As you may be aware, all care for transgender kids under the NHS is currently provided by GIDS, the Gender Identity Development Service. At present, this operates mainly from the Tavistock & Portman Trust in London, often referred to as just “The Tavistock”. I say “at present” because a recent independent review (Cass, 2022) led to the recommendation for it to be closed and replaced with regional centres.
Our child has been on the waiting list for this service for approximately two years, after they began experiencing gender dysphoria1 during the Covid lockdown in 2020, which is when they also came out as transgender. At the time of writing, they are 15.
We did what I think most loving parents would instinctively do which is to tell them (as we always have) that we love them no matter what, no matter whom they love or how they identify. That simple position is never, ever going to change.
I’m not going to include a lot of detail about them here, because their life is private and their own to share (or not) as they choose but suffice to say we had reason to be worried about their safety. The last thing on earth any parent wants is for their child to be in serious distress and, of course, you want to do anything and everything you possibly can to keep them safe.
We switched to their preferred pronouns, as well as a new, chosen name and started to educate ourselves about what this journey might entail. We wanted to make sure we could get expert advice and support so, with GIDS being the only option on the NHS, we requested that our GP make a referral. It was also a way of tangibly showing our kid we took their feelings seriously and weren’t dismissing how they felt. We were advised (as we pretty much expected) that the waiting list was long and we shouldn’t expect to hear anything for 2 or 3 years.
In the meantime, we were signposted to support groups of parents going through a similar experience, such as the one run by Mermaids, and others. There were lengthy vetting processes (which I suppose is understandable when granting access to a group where private medical information might be discussed) but I was eventually accepted into some of these, including the UK-based group on Facebook I was recently ejected from.
I was looking for advice, information and reassurance, and the parents who had already trodden this thorny path seemed the obvious people to talk to. No doubt, I thought, the questions and fears we were having must have also been experienced by many of the members of these groups. They would surely be well versed in the details and dilemmas and be able to offer insight.

The norm in these groups is to introduce yourself in a post that briefly tells your (anonymised) story, so I did this, and found myself being roundly congratulated for being such an understanding dad and for supporting and affirming our kid. I assumed they were mainly focussed on being kind and welcoming as obviously they didn’t really know anything about us beyond the few paragraphs I had written. But it felt good to be told we were on the right path, that we were doing the right thing by our child.
At first, I spent time reading and listening to other parents, and going through many of the existing posts and discussions. I didn’t want to be that annoying guy who asks questions that are answered on the first page of the FAQ or demand effort from other parents, who almost certainly have their own worries, and limited time to spend educating me.
Everyone I encountered seemed to be very genuinely just trying to love and support their kids, to get them through this difficult time in their lives and help them find their place in the world so they could be happy.
As I read more over the following days and weeks there were quite a few posts from parents excited to report that their kids had got puberty blockers, started on hormones or were going in for “top surgery”2. They reported effusively on the joy, even euphoria the kids had about these developments, which sounded very positive.
We’d heard our kid mention some of these treatments and, although it is still unclear which, if any, they may eventually want or choose, we wanted to understand fully what is involved, and to do our own “due diligence” on their risks and benefits. If it’s our responsibility as parents to keep our kids safe, then that includes helping them navigate what might be very difficult decisions and we wanted to be sure we could help them find accurate information to do so.
I’m not going to lie – it wasn’t always an easy read. Treatments like mastectomies and medication that leaves your kid sterile are not things anyone should take lightly. But, of course, neither is the prospect of losing your child entirely. And we all know that very often in life there is no perfect answer, only a “least worst option” or a “best guess, based on what you know at the time”.
That said, when I consistently heard the phrases that are thrown around ubiquitously like “completely safe” and “fully reversible”, my naïve expectation was that there must be a bunch of big studies with large numbers of patients and clear-cut statistical results showing strong benefits.
Of course, as soon as you stop and think about it, you realise that running an experimental study on large groups of adolescent kids would present a lot of ethical questions and I couldn’t immediately picture how that might work. However, I figured there must be a sensible answer, as I didn’t think it was remotely plausible that respected authorities would make these kinds of statements without some genuinely compelling evidence.
I hadn’t been able to find that yet, but my hope was, in these groups full of parents who had been on this path longer than us, we could shortcut the process. I was anticipating that, if I described my fears in these places, someone would likely appear in the comments and say something like “you’re not alone - I had the same worries and here is a link to the research that helped me feel the risks were justified”. I wasn’t expecting certainty, or that every parent and child would have made the exact same choices, only that we might be able to follow their logical process through, look at the same materials, and use that information to help our kid make their decisions.

A short tangent about me: I write software professionally, but I have a wider background in science – I studied Biotechnology at university and spent some time after that working in scientific research. Lurking somewhere in the annuls of an obscure scientific journal, my name is on a published research paper containing the work I did back then.
No doubt that background has shaped my thinking but, for whatever reason, I don’t know of any better way to assess evidence and arrive at an objective answer than using a scientific approach. Data doesn’t have an opinion: it is neither “good” nor “bad”. You look at it critically, you ask questions about how it was collected, and you draw only those conclusions that can be supported by the evidence. There might be more than one possible conclusion, and all should be challenged for robustness and to root out any invalid logic. Results that contradict previous outcomes are just as important in uncovering the truth as evidence that confirms them, arguably even more so, because they might be indicating something you have missed. You only approach an answer that is considered “settled science” when there is a strong weight of evidence from multiple sources.
Perhaps I was overly optimistic about what I could get from these support groups, but it didn’t turn out to be as simple as I had hoped to find the information I was looking for. The most common response I received was a non-answer: variations on “better a trans kid than a dead kid”. That is, of course, a statement no reasonable parent could disagree with, but neither is it at all helpful in navigating the actual complexity of the situation.
The issue for me wasn’t whether or not my child identified as trans; it was whether or not they chose a medical path that could hurt them or that they could later come to deeply regret. Whether or not to have any particular treatment is a choice independent of identity, and one that should take into account a realistic assessment of the risks and benefits.
When I asked in these places about these more difficult questions and whether anyone else was also troubled by this kind of thing, I found not acknowledgment or validation this time but something more like disdain and suspicion.
As with a number of similar communities, the Facebook group I was part of holds up the guidelines created by the World Professional Association for Transgender Health (WPATH) as the best practice and some people pointed to this. I can see why parents would feel they should be able to trust such guidance: I felt the same, initially; surely these were the best experts the world had to offer on trans healthcare, so I could take what they said at face value?

Maybe it was the latent scientist in me, but I became curious about the exact details – I wanted to be able to quote some numbers, if needed. I imagined that once I drilled down, maybe I’d be in a position to say something like “ah yes, 75% of kids in this major study saw a massive improvement in dysphoria and side effects only occurred in 0.5%” or something along those lines. That would reassure me, and I could explain honestly to my child why they could feel reassured too if they wanted to take that route. I could arm other parents with those details as well.
So, I started with the WPATH guidelines (Coleman, 2022). This is a document that covers clinical guidance rather than setting out any evidence itself, but there is a long list of references, spanning the wide range of topics the guidelines cover, and I began to look at those.
If our child followed the typical route in GIDS, treatment would start with puberty blockers, which are widely referred to as completely reversible. So, I thought, there must be evidence that shows this, and it would be good to know what the numbers are there. For example, I presumed they must have monitored the outcomes of kids who chose to stop taking blockers, to see if they returned to the normal course of puberty.
However, as best I can tell, the case for the safety and reversibility of puberty blockers appears to rest on two things:
Firstly, that the same medication has been used clinically for suppressing very early (precocious) puberty in young children, typically under age 8. I understand the logic, because these kids do appear to go through normal puberty when they stop taking the blockers (Kim, 2015). However, it is a fundamentally different developmental phase and usage of the medication.
As anyone who has been through it knows, puberty is an incredibly complex developmental time and the assumption that the effects in a 7 or 8-year-old are the same as in a 16-year-old are, at best, extrapolation. The published literature does also point to some potential health issues when continuing the use of blockers beyond age 11 (Kim, 2015). That is obviously concerning but, even putting that to one side, it certainly doesn’t offer any actual proof it is completely safe or reversible in an older age group.
The second set of evidence cited explicitly looks at usage in adolescents for the treatment of gender dysphoria. In this area, as best I can tell, the evidence appears to rest very heavily, if not entirely, on a research study carried out in the Netherlands, colloquially referred to as “The Dutch Study” (De Vries, 2011).

A lot has been written about this, and I am not going to try to cover all the details here. But essentially what I was reading indicated that while it does show some benefits of puberty blockers and hormones in the small group of children that were studied, there is a significant list of reasons why it is questionable whether it applies to the typical kids seen at GIDS, and to our child specifically. It’s also worth noting that it doesn’t examine those kids who stop taking blockers at all.
I wasn’t taking any of this at face value, I wanted to talk about the specifics – respectfully, of course – in these groups that I was part of. If I was finding this stuff and worrying about it, then I imagined other parents must have done the same. Maybe some had already found more evidence. Maybe the parents whose kids were already at the Tavistock would have some materials they could share – leaflets or less well-known research, or something. Or maybe we could investigate together.
I’d found a number of published papers reviewing the findings of the Dutch study and the treatment protocol based on it, which seemed to raise some important questions about the findings and their potential flaws. I posted a link to one of these in the group (Biggs, 2022) and asked – genuinely, as carefully and sensitively as I could – whether what it said was accurate. I asked whether there were reasons why these viewpoints were flawed or could safely be disregarded and, if so, where I might look for additional evidence.
However, I was contacted shortly afterwards by a group admin to tell me my post had not been permitted due to the fact that the research had, apparently, been funded by “hate groups”.
That was alarming and, to be honest, I felt a bit foolish that I had missed this if it was so obviously disingenuous. I wanted to know more and so asked for details (see conversation below).
I was expecting them to answer by doing something like pointing to the small print to show it said it was funded by group X, and that then if you looked at the webpage for the group it would say “eradicate trans people!” or something awful like that.
This was the conversation:
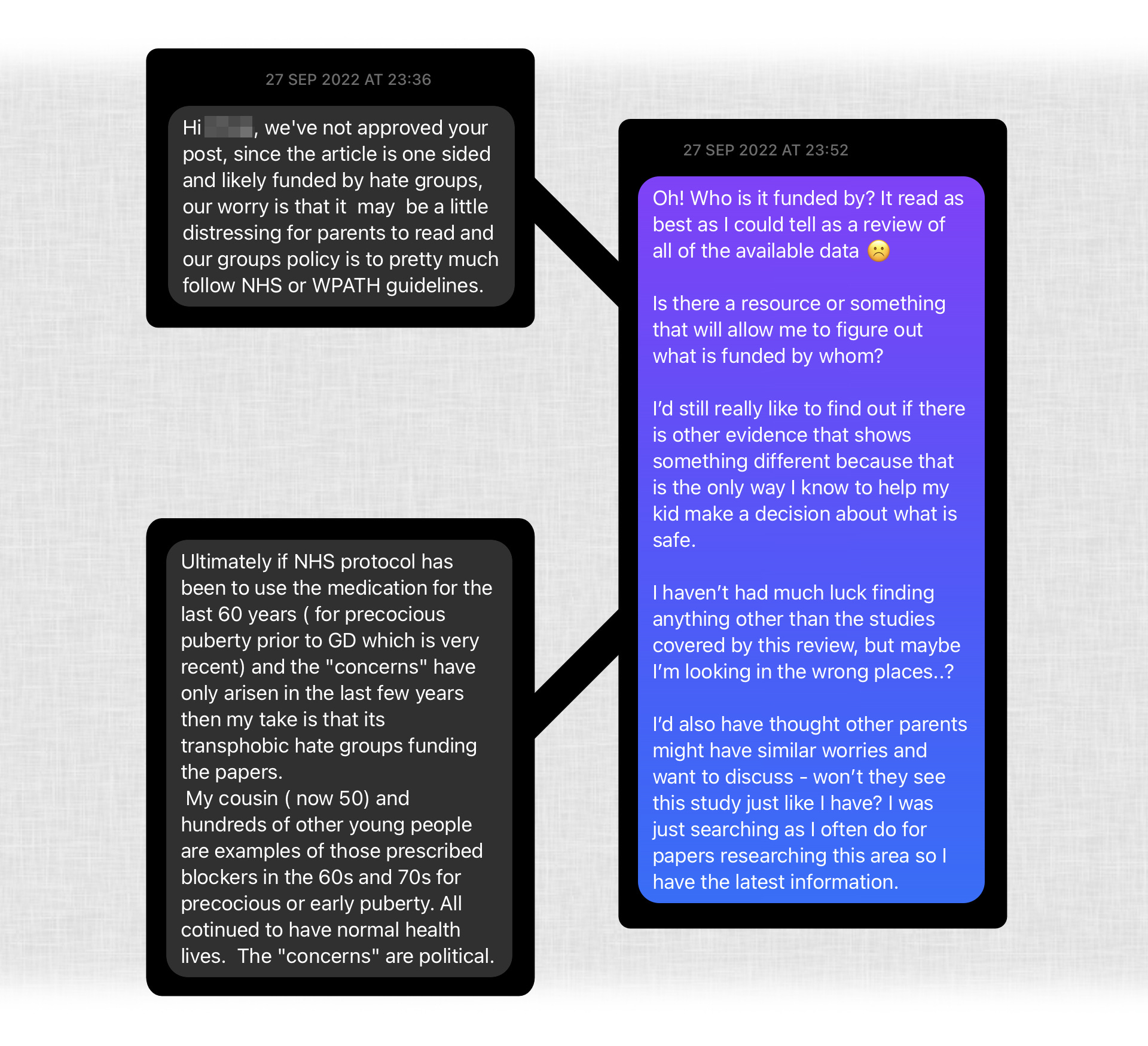
As you can see, the refusal wasn’t based on any actual evidence it was funded by “hate groups”, it was assumed that simply because it didn’t reinforce the group’s existing accepted viewpoint, it must therefore be motivated by transphobic hate and automatically have no merit. And discussion even of its existence was not permitted.
This seems to me an entirely blinkered position to take. I was very willing to hear how it might be subject to bias, or how the logic might be flawed, or that I had made a mistake and missed something specific in the paper.
But this way of thinking means that you can fundamentally never consider that you might be wrong. That no amount of evidence that might accumulate would ever be enough – the fact that it didn’t say what you wanted it to was taken as proof that it was unreliable and a result of bad intentions. And therefore nothing could ever challenge your existing position.
Surely, I thought, that was a dangerous approach, when what really mattered for our kids’ safety was getting to the actual truth?
I asked for more clarification:
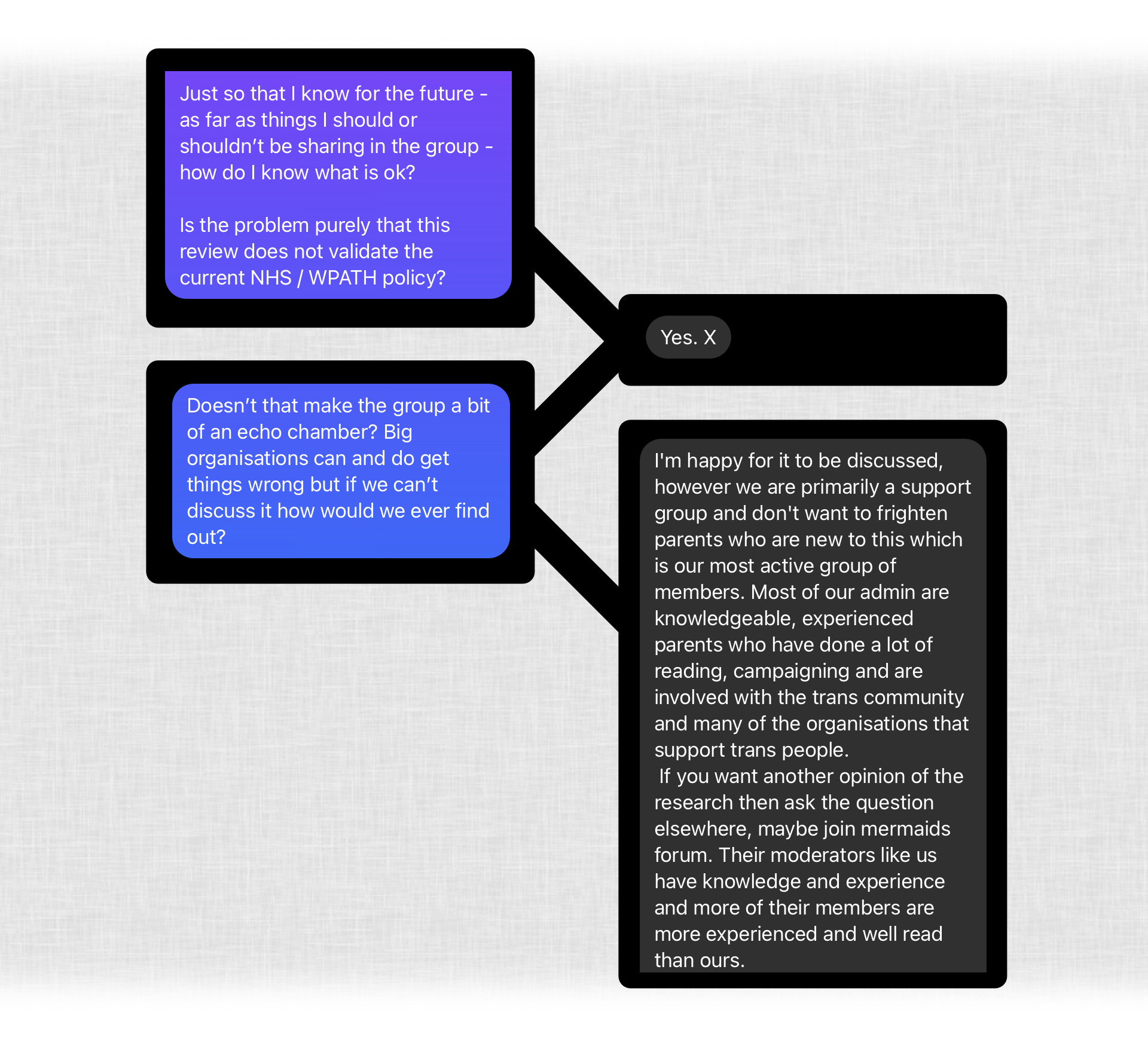
I’m not sure how stopping me from posting equates to being “happy for it to be discussed” but, essentially, their stance was that it is more important not to “frighten parents” than for them to have accurate information. I’m pretty sure that most parents, like me, would say they couldn’t care less about their own comfort or upset when it comes to the safety of their child. I’m not going to risk doing something harmful to my child just because it might be upsetting to hear the facts.
I am very sympathetic to the idea that it could be upsetting for parents to consider this if it might cause them to question whether the path their child was already on might be wrong or harmful. But, if that was the case, surely those parents and kids needed this information more than anyone?
For what it’s worth, I did also try the Mermaids’ group – as you will see later. But the admins of this group were not happy with me now, and went on the offensive.
I’ve seen a lot of what I think of as the “Emperor’s New Clothes” tactic being used recently, and this is an example. Instead of offering actual evidence to support a position, an attempt is made to shame you into agreement by implying (or outright saying) that if you are not able to see that this is obviously true, you must be blinkered or stupid, or you have been duped.
Or sometimes it’s dressed up as sort of back-handed compliment – “oh surely someone who is as smart as you knows this”. To me, this smacks of someone who is simply parroting what someone else fed them and who has not thought critically for themselves.
I should probably have quit the group there and then, but instead I justified my existence to this person and stayed because I still felt there must be parents having the same concerns as me and I wanted to be able to connect with them.

I continued to do my own research, listen to parents’ experiences in the group and respond when I could to parents who looked like they had similar fears to mine.
A little while later, someone else posted (rather nervously) on the group that they had seen that there appears to be a correlation between teens identifying as trans and those diagnosed with Autistic Spectrum Disorder (ASD) and did anyone know if there was a connection or explanation.
I replied with some information I had seen confirming those stats, based on the Tavistock’s own publication (Spiliadis, 2019) which demonstrates that there does appear to be an unusually high proportion and that I thought it was valid to ask questions about it. I said I would like to know the answers too, as our child was recently diagnosed with ASD. There was absolutely no implication that either being autistic or trans was a negative thing, only that it was reasonable to wonder why this pattern occurs. Many of the responses (probably most) were more or less accusations of transphobia saying it was not ok to even ask such a question.
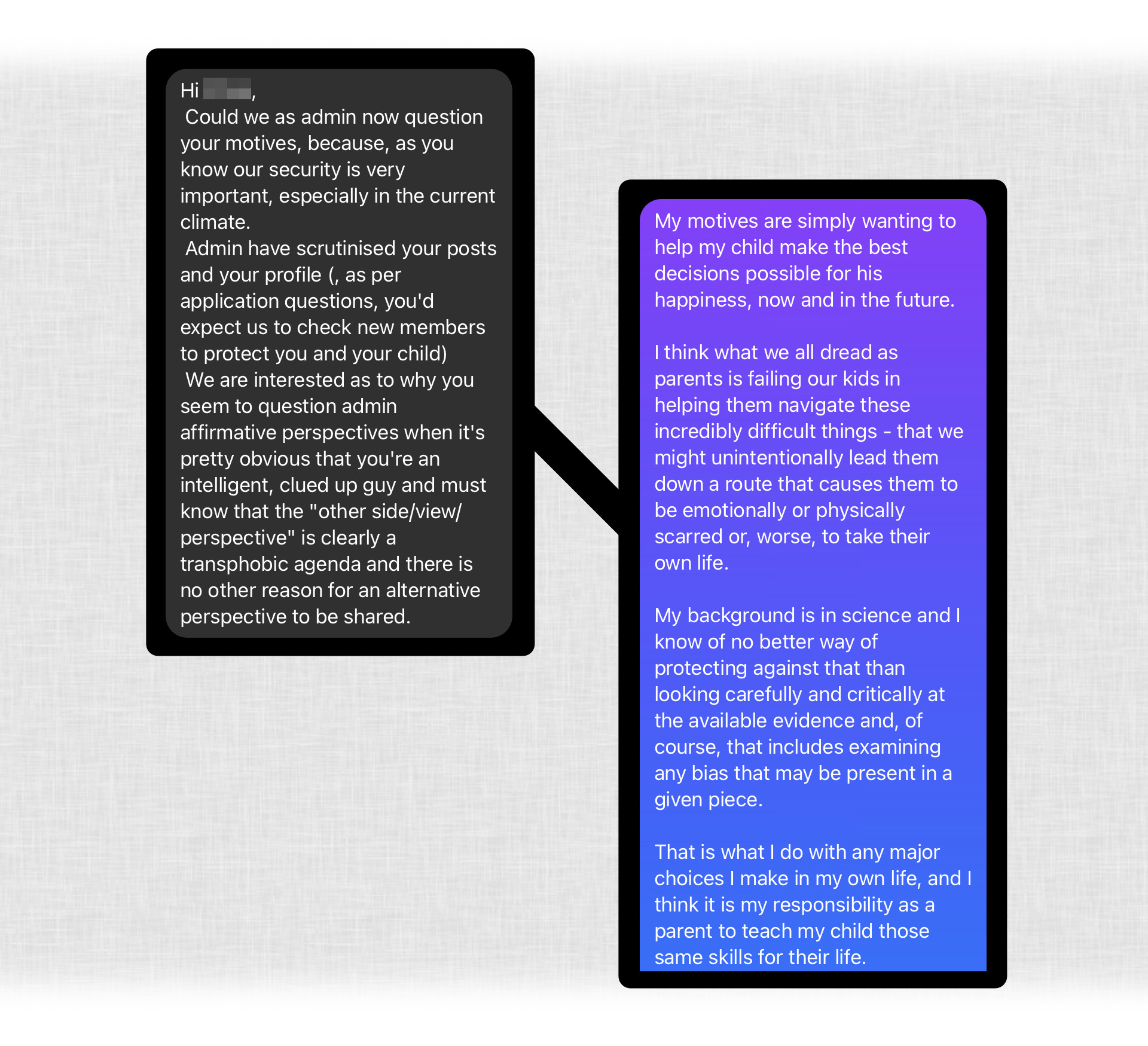
Again, I was contacted by a group admin, this time saying they had had complaints from other parents about my “apparent ‘2 sided’ views” on this. Why looking at two sides of an argument would be considered a bad thing, I don’t know.
As per the below conversation, I was a “concern” to the admins because I continued to “question things”. Apparently even though the information I mentioned was directly from the Tavistock, it was still “the transphobic media” that were “throwing out this crap”.

I was simply too … stubborn? stupid? to acquiesce to the admins’ obviously greater experience and knowledge. Even though they spouted baseless claims like the above, stating that being trans is genetic, which, unless I have really missed something huge, there is no evidence for whatsoever. These are the people who “know their stuff” that I should be deferring to!
As you can see, they also had another dig through my social media and came back saying I rang “alarm bells”.
Again, I should probably have taken all of this as a very clear cue to leave this place but, once again, I explained how (hard as it may be for them to fathom) I am genuinely just a parent who wants the actual truth so they can do the best thing by their kid. And I don’t think my page is especially political – I pointed out that I don’t share much on trans rights because a) it can be very divisive and b) it’s difficult to do so without revealing or at least implying information about our kid.
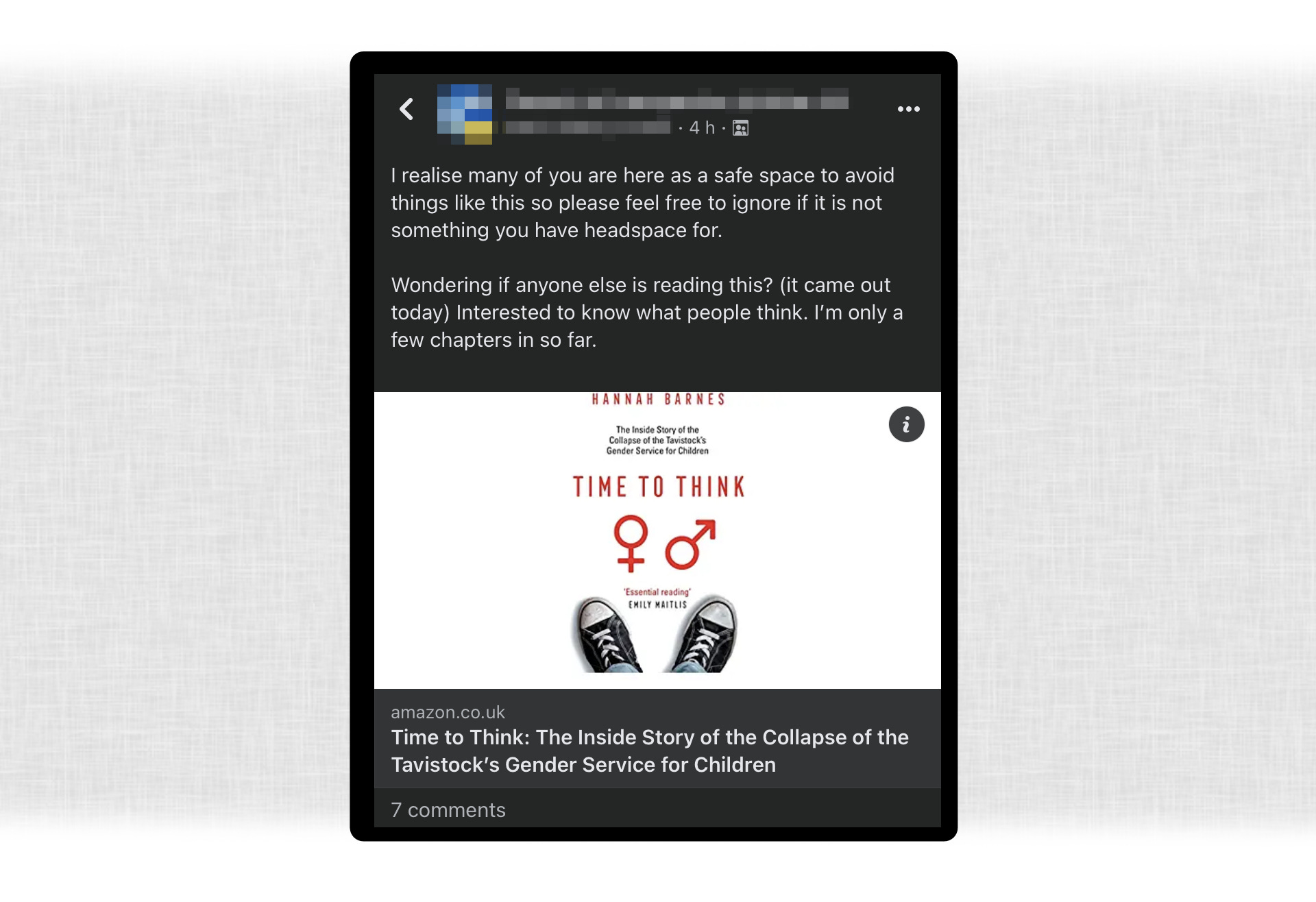
Fast forward to February 2023 (as I write, last month), and Newsnight journalist Hannah Barnes published her book “Time To Think” covering the details of her research into GIDS at the Tavistock. Given that pretty much everyone in the group either had kids at the Tavistock or on the waiting list, you’d think this book would be of real interest. Even if it contained accounts that did not match group members’ own experiences you’d think that people would still want to know what it said. If it contained outrageous lies, then surely they would want to set the record straight?
But I guessed it might be contentious because of my previous interactions with the admins, so I decided to contact them first and ask about discussing it within the group. Here’s how that conversation went:

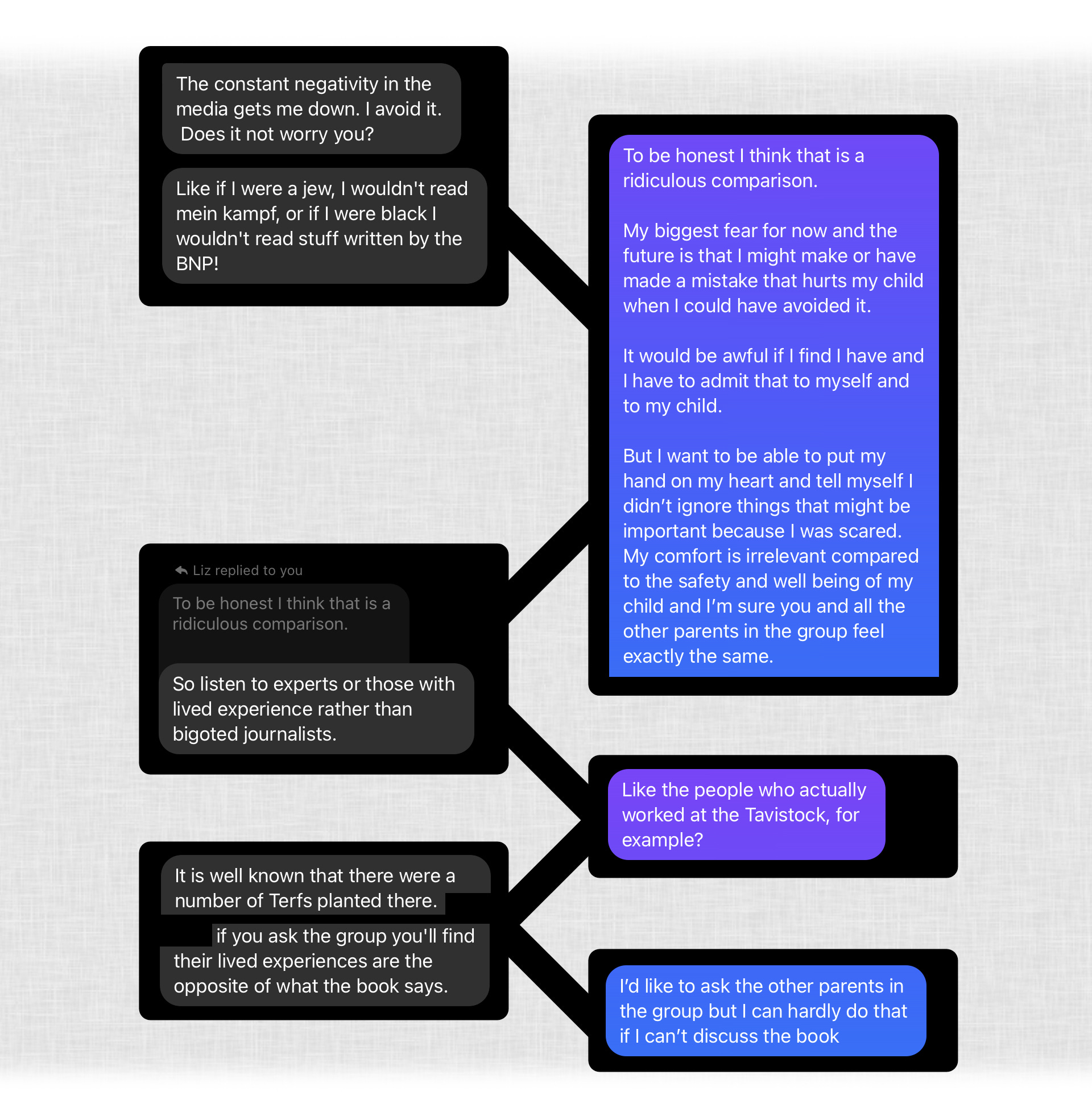
I didn’t genuinely think this admin was suggesting the book was fabricated but, truthfully, I couldn’t see any other way you could discount what was in the book. If you accept that Hannah Barnes spoke to the 60+ people from the Tavistock she mentions, and that the quotes are at all accurate, then there is real cause for concern and to at least ask some questions.
And, obviously, it is utterly awful what happened to Brianna Ghey but it is absolutely nothing to do with this conversation. Rather than offering actual discussion or evidence, I was essentially told that the “clever” media and their bias was beyond my understanding, and that I was not even as informed as the 11-year-olds that they apparently teach.
And then it got more ludicrous. Apparently, Hannah Barnes is the new Hitler, and it is “well known” that TERFs (Trans Exclusionary Radical Feminists) were “planted” at the Tavistock:
I’d almost completely given up by this point but, after some more to-and-froing, they suddenly surprised me by saying I could post about it after all. So, I did and, after admins had vetted and approved it, I began to have a few conversations in the comments.
With one exception (see later) I’m only sharing my own posts from within the group as, when I joined, I agreed not to do so, to protect the privacy of parents and kids there. But this was my post:
A lot of the replies were very similar to the admin response: that she is a “well known transphobe” and that they wouldn’t read it. That’s ultimately their choice, and I was mostly interested in whether there were any parents that were casting their net a little wider, like I was. But I did ask for any examples they had of problematic things she had previously done or said. The only item volunteered was a link to an article about the Newsnight report she was involved in. That did not itself offer any actual quotes or concrete examples, and seemed to rest on the assertion that questioning the current medical model at all was itself innately transphobic.
But before those conversations could get very far, the admin came back again to complain about the post, even though they had just explicitly approved it, saying it now broke the rules. I don’t think the rules had changed in the few hours between these events but, to be fair, I wasn’t monitoring them.
Apparently now the link was transphobic:
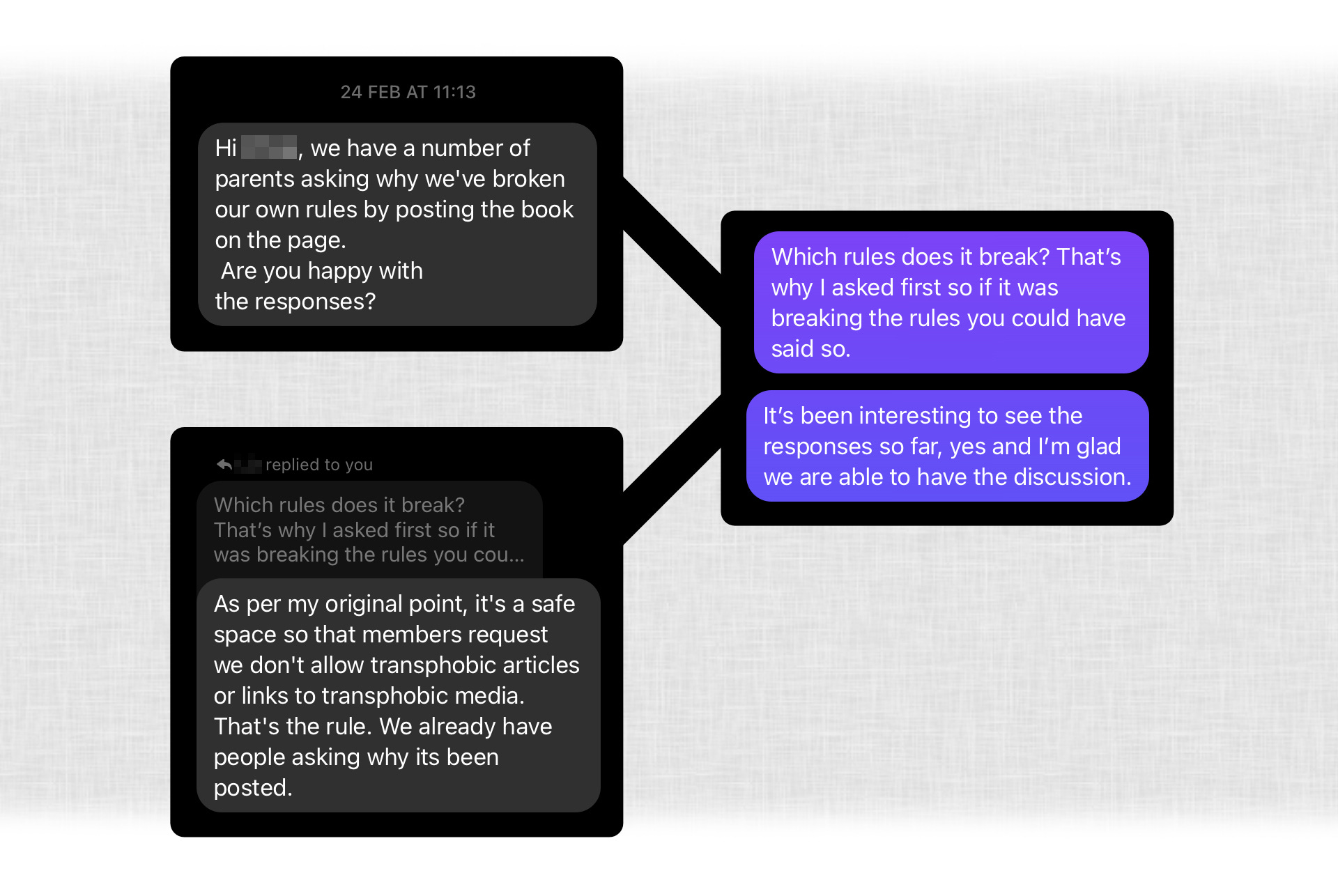
Again, it was clear that the priority was not upsetting parents, rather than allowing parents to have the important discussions that are so needed about the safety of children. And a completely unqualified assertion that the book is transphobic.
Shortly after this, they decided to remove me from the group, and that is, of course, their right as group admins. Apparently, any other “supportive” parent would “know” this was transphobic, so I presumably am not a supportive parent:
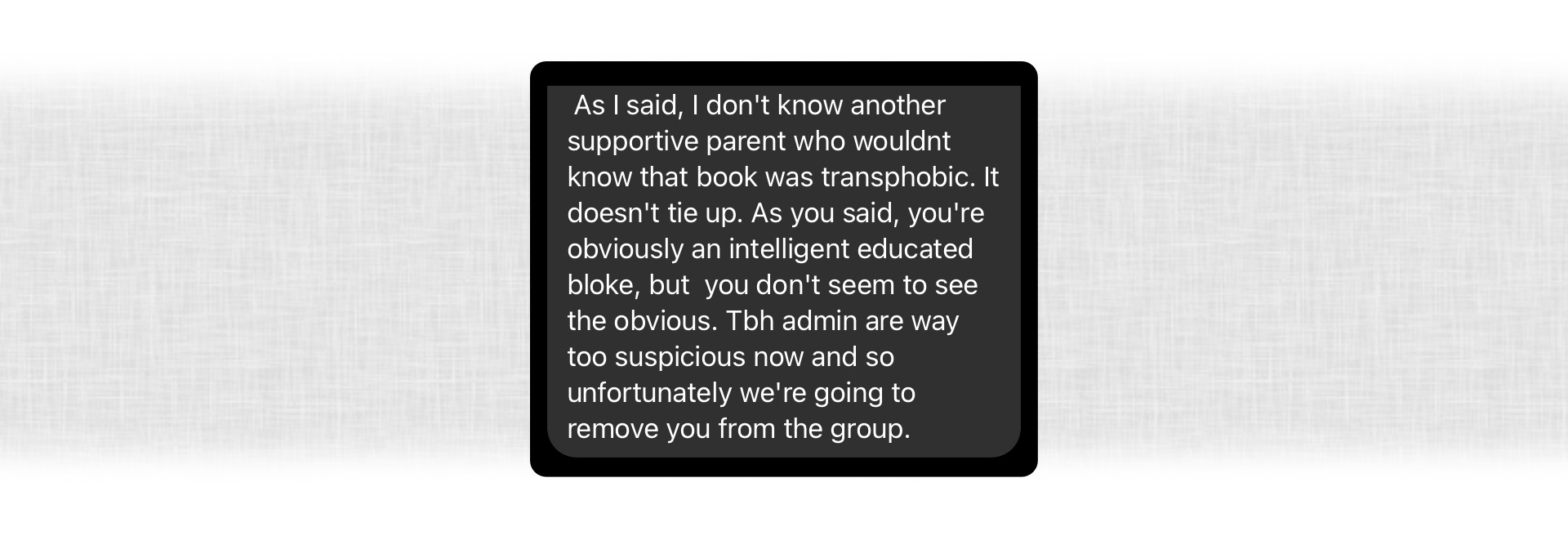
According to another member who remained and reached out to me, they announced that I had been removed for “reading transphobic literature”. A warning, I suppose, to anyone else who might ask any similar questions.
I don’t see it as a huge personal loss to be out of the group, because I think it is a huge echo chamber where critical thought and discussion can’t really happen and, from that perspective, it couldn’t give me the support I needed. But what does make me angry is the thought that there are no doubt parents in the group who are wrestling with the same things and this is a very public indication that they should not ask.
Worse than that, I worry that there may be parents who aren’t aware there is more information to consider, who now may not hear about it at all. Perhaps it wouldn’t have made the slightest difference to their decisions. But it’s also possible it might have helped them spot and avoid something that they later come to realise has hurt their child. However “upset” they might have been by seeing a link to a book, I don’t think it will possibly compare to how they would feel should that eventuality unfold. I hope it doesn’t, for theirs and their kids’ sake.

This way of thinking is not confined to one group. As you may recall, the Facebook group admins suggested I try the Mermaids parents’ group as a place for critical / evidence-based discussion, which I did. However, I received a very similar response there:
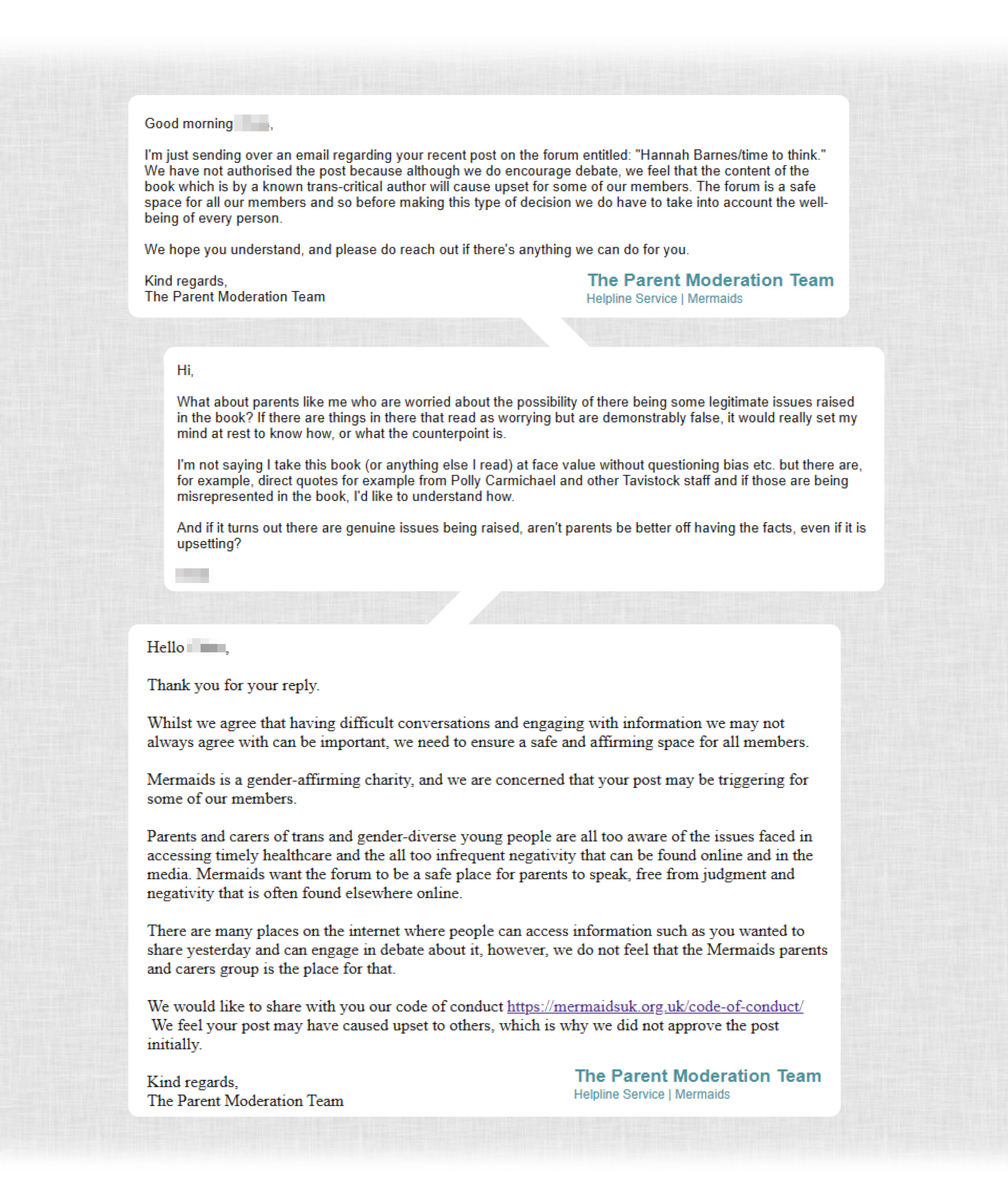
Again, the avoidance of “upsetting” parents is the priority rather than providing what might be critical information. And anything that does not reinforce the existing stated position is considered harmful, and you cannot discuss it at all.
What is especially frustrating is that this blinkered way of thinking very much echoes some of the issues that Hannah Barnes’ book describes as occurring within the Tavistock. Many people she spoke to indicated that raising concerns resulted in direct or implied accusations of transphobia, or individuals being branded as difficult and that, as a result, many were afraid to speak up. That there seemed to be more anger over how it made staff feel than whether there were legitimate issues affecting the safety of children.
I do understand that, for some parents, they want a place to avoid these discussions, a safe space where they can go for reassurance and nothing else. But the problem is that this is not how these groups are presented. Parents are signposted to these places for information and advice whilst awaiting their future appointments with GIDS, which is typically not going to happen for years. In the meantime, if they are under the impression that they are getting balanced information, and they see no visible challenge of the data and no concerns raised, they are potentially being lulled into a false sense of security, feeling informed when they are only getting a very distorted representation of the science.
I saw many parents talking about having gone to GenderGP3 because the wait for GIDS is so long. That is understandable on many levels – having to wait years for an appointment is clearly not anything approaching a properly functioning service. However, it is also clear from the comments I have seen from parents in the group that GenderGP grant access to medication much more quickly and with fewer checks. It certainly didn’t sound like they were filling in many gaps in information or highlighting the risks, though I could be wrong - again, it would have been nice to be able to ask other parents. Going into an even less rigorous process with a false sense of confidence about the safety of treatments is obviously even more dangerous.
As I have tried to get across, I am not assuming that I have been able to find all the evidence that is out there. I am still, truly and honestly, hoping there is more, and it is simply my research skills at fault here. That being said, the fact that the interim Cass review (Cass, 2022) notes that “there are significant gaps in the research and evidence base” and that the NICE evidence reviews that fed into it found that that the existing evidence is “very low certainty” would suggest there are at least some areas where there simply isn’t much to go on (see References for details).
There were many parents in the group who said their kids were already on the treatment path at GIDS, and their reported experience of the service was pretty exclusively positive. However, I did notice that these same parents were adamant to reinforce statements like medication being “completely safe” and “fully reversible”. I don’t see how they could therefore have been told anything else by the professionals they saw – if they had, why would they say this?
That being the case, I wonder how they would feel if they understood that this is an overstatement of the certainty around the treatment their kids are on. I wonder whether if it had been presented more as something experimental and unproven, with unknown risks and less clear evidence of benefits, whether they would still have made the same choice. I don’t blame them for trusting those in an apparent position of authority – they should be able to do that. But, as upsetting as it would obviously be, they have the right to know if the science was misrepresented to them. If you are not given accurate information, you are not giving informed consent.
A parting note: not long before I was barred from the Facebook group, I saw I had had a reply from Susie Green, former chief executive of Mermaids. I don’t know if it was coincidence that I was removed shortly afterwards, but I did not get a chance to respond.
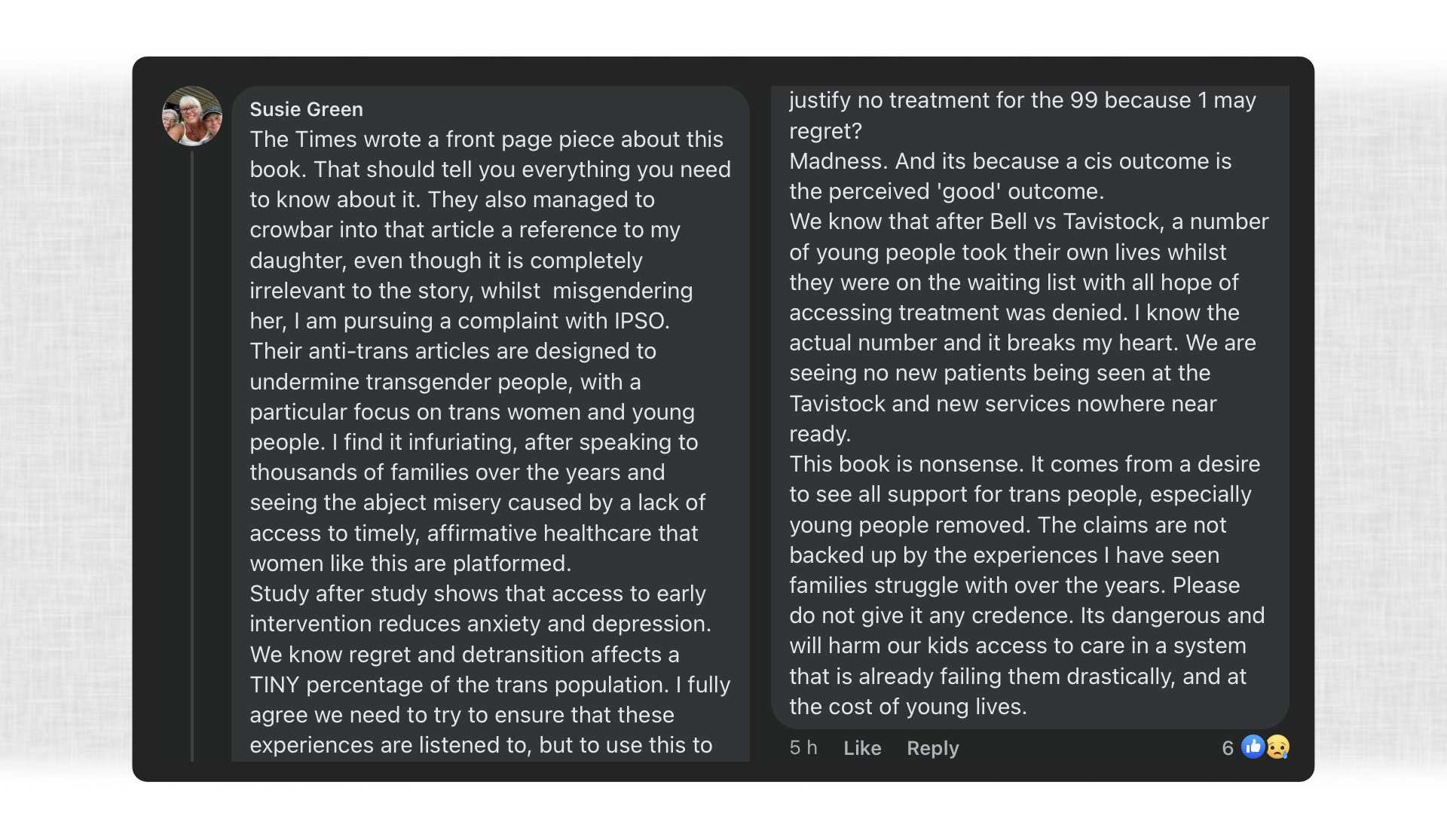
As I said above, I agreed not to share content from within the group, in order to protect the privacy of parents and kids there. I would never post anything that publicly outs someone, especially not a child, but I don’t think that applies to this particular comment, as it is someone already well known in the public domain, and the child in question is now an adult and has frequently shared details publicly. As an individual who is highly influential in groups like this, I think it is informative to see what she had to say.
Obviously, we are all aware that the media can have and does have bias, but I’m not sure how the fact it is on the front page of The Times is supposed to tell me “everything [I] need to know”. As far as I am aware, there is not a long, well-established history of complete lies being published on the front page of The Times4. I think this is another Emperor’s new clothes thing where if I am so stupid that I don’t know, I am obviously beyond help.
I’d have liked the chance to ask about the statistics she quotes and the data that underpins it, which was essentially my original reason for posting, and for joining the group. She says that “study after study [show] that access to early intervention reduces anxiety and depression” and I have genuinely looked hard for information like this. There are a number of studies that show positive results for affirmative care in various ways BUT, in similar ways to the Dutch study example above, there are often question marks over the quality of the data and whether it applies to the current cohort of kids. From what I’ve seen, the data to back this up is far thinner and less conclusive than the way it is presented. I would genuinely love to be corrected and that is why I wanted to ask. But apparently that is not allowed.
As far as suicide statistics go, it sounds like she has some additional information that is not widely available, and I would also have liked the chance to find out more about that. If there was a spike in waiting list suicides after the Bell vs Tavistock case that would obviously be something that ought to be investigated and understood. But I didn’t get the opportunity to ask, so if that might have influenced our choices, I don’t get to find out how.
From these comments, it seems to me that she very much promotes the same line I’ve seen repeatedly now: if something or someone asks questions at all, it is transphobic; it cannot be tolerated and should not even be discussed, not even to debunk it.

Evidently, none of the people I’ve spoken to who espoused opinions on what Hannah Barnes’ book contains have read it. I can of course understand that many people won’t have the desire, energy or time to do so but, fundamentally, if you haven’t read a book, your opinion on it is not meaningful.
I have read the book, and it does not at all support the notion that “a cis outcome is the perceived ‘good’ outcome”. It does not argue to remove support from trans people, nor does it argue against the existing medical pathway remaining available. It argues for greater resources and better care for trans people. It supports the case that more time and resources should be made available for exploration of complex cases, such as individuals with a history of abuse or trauma, or those with co-morbid conditions. It argues for greater rigour in presenting the risks and benefits of treatment to those who are deciding whether or not to have them. It includes plenty of examples of positive cases of transition through the Tavistock and does not demonize staff or trans people, nor does it in any way try to say that every patient had a bad experience.
It does, however, raise a number of difficult questions that need an answer if we want to be sure we aren’t inflicting avoidable harm on potentially large numbers of young people.
There may well be ways in which the book is demonstrably wrong and I would genuinely like to know what the counterpoints are. An excellent way to find out would be to talk to people in groups like the ones I was part of in a rational, coherent way, to get to the detail of how and why it is wrong. However, it seems that is not something that is permitted and, rightly or wrongly, that rather leaves me with the impression that there simply weren’t any valid objections to raise.
My advice to parents of trans kids looking to these groups for support is this: if you think there is a one-size-fits-all treatment for every single trans kid, and if you want somewhere to be patted on the back and uncritically told you are doing the right thing, then these places will make you very happy. However, if you want to get to any kind of objective understanding of the risks and benefits your child may face, then don’t be deceived: you’ll need to look elsewhere.
Scientific Parent Of A Trans Kid, March 2023

References
Barnes, H. (2023). Time to Think: The Inside Story of the Collapse of the Tavistock’s Gender Service for Children. Swift Press.
Biggs, M. (2022). The Dutch Protocol for Juvenile Transsexuals: Origins and Evidence. Journal of Sex & Marital Therapy, Advance Online Publication, 1–21.
Cass, H. (2022). The Cass Review. Retrieved from https://cass.independent-review.uk/
Coleman, E. R.-B. (2022). Standards of Care for the Health of Transgender and Gender Diverse People, Version 8. International Journal of Transgender Health, 23(S1), S1-S260. Retrieved from https://www.wpath.org/publications/soc
De Vries, A. L.‐K. (2011). Puberty suppression in adolescents with gender identity disorder: A prospective follow‐up study. The Journal of Sexual Medicine, 8(8), 2276-2283.
De Vries, A. L.-K. (2014). Young adult psychological outcome after puberty suppression and gender reassignment. Pediatrics, 134(4), 696-704.
Evidence review: Gender-affirming hormones for children and adolescents with gender dysphoria. (2022, July 26). Retrieved from https://cass.independent-review.uk/wp-content/uploads/2022/09/20220726_Evidence-review_Gender-affirming-hormones_For-upload_Final.pdf
Evidence review: Gonadotrophin releasing hormone analogues for children and adolescents with gender dysphoria. (2022, July 26). Retrieved from https://cass.independent-review.uk/wp-content/uploads/2022/09/20220726_Evidence-review_GnRH-analogues_For-upload_Final.pdf
Kim, E. Y. (2015). Long-term effects of gonadotropin-releasing hormone analogs in girls with central precocious puberty. Korean Journal of Pediatrics, 58(1):1-7.
Levine, S. A. (2022). Reconsidering Informed Consent for Trans-Identified Children, Adolescents, and Young Adults. Journal of Sex & Marital Therapy, 706-727.
Media Bias Fact Check: The Times UK and The Sunday Times. (2023, March 7). Retrieved from Media Bias Fact Check: https://mediabiasfactcheck.com/the-times-of-london/
Spiliadis, A. C. (2019). ‘Taking the lid off the box’: The value of extended clinical assessment for adolescents presenting with gender identity difficulties. Clinical Child Psychology and Psychiatry, 24(2), 338–352.
Footnotes:
There is debate over the exact definition of this term, as well as whether or not it constitutes a mental disorder. The Diagnostic and Statistical Manual of Mental Disorders (DSM) is a reference book on mental health and brain-related conditions and disorders, published by the American Psychiatric Association (APA). The latest version (v5, May 2022) describes Gender Dysphoria as clinically significant distress or impairment related to gender incongruence, which may include desire to change primary and/or secondary sex characteristics.
In case you are not familiar with this term, it is the name used for an elective double mastectomy – the surgical removal of both breasts.
GenderGP is a private, online provider of transgender healthcare.
According to media reliability and bias rating site, mediabiasfactcheck.com, it is rated as right-centre leaning and high credibility (Media Bias Fact Check: The Times UK and The Sunday Times, 2023).
Just to add, I am having a stab at setting up a facebook group that allows the kind of discussions that were not permitted in the spaces I've found so far. No idea how easy it will be to get a critical mass of people to join, but I'm giving it a go.
https://www.facebook.com/groups/237822368721915
Thank you for writing this. I too am a Ph.D. scientist, and have asked trans activists to provide suggestions on where to find the supposed “vast body of scientific literature” supporting their assertions. I also asked in good faith- I like to believe I would be persuaded by data.
But every study that I was referred to was either flat out wrong (basically all the genetic studies) or at best extremely weak (small sizes, short time frames, bad or missing controls, huge drop-out rates with no follow-up, barely significant signals based on self-reported feelings, etc.) The text of these papers often contain statements that are wildly overblown or simply not supported by their own data.
So I experienced the same reaction you did. Eventually I realized I was engaging religious zealots. I simply was not going to convince them with facts, and of course they will be hostile to any questions regarding their faith. This isn’t surprising, as this is a group of people who believe in a metaphysical gender that can be expressed independent of a physical body. That is a religious belief, not science. And the priests (aka moderators) don’t want you or I leading anyone in the flock astray with pesky science questions.
It would all be relatively harmless foolishness if it wasn’t leading to permanent mutilation of a generation of young people.