


Parent Summary: Puberty Suppression in Adolescents With Gender Identity Disorder: A Prospective Follow-Up Study

Original authors: Annelou L.C. de Vries, MD, Thomas D. Steensma, MSc, Theo A.H. Doreleijers, MD, PhD, and Peggy T. Cohen-Kettenis, PhD.
DOI: 10.1111/j.1743-6109.2010.01943.x
What is a “Parent Summary”?
My aim in writing this is to present the information contained in the named study in a way that is accessible to a wide range of parents with trans kids, who may not be familiar with digging through formal scientific papers themselves.
I have deliberately avoided expressing any opinion on the content, though I may write other pieces that do in the future. But here, I am solely aiming to present what the authors say in more straightforward language. It’s not devoid of specialised terminology, but I have tried to make it so everything you need to understand the paper is in one place, with additional data in appendices where I think it is helpful.
I hope that reading this will allow parents to feel confident commenting on the content of a study in further discussion and to assist their child(ren) in making decisions about the treatments discussed.
The full version of the paper can be found at https://pubmed.ncbi.nlm.nih.gov/20646177/ or searched online using the above DOI details1.
If you think I’ve missed or misrepresented anything here, please let me know, and I will endeavour to update this article.
Please note: there are certain parts of this study that I personally believe to have significant limitations or inaccuracies - I am not addressing this here, but rather in a separate document, to maintain clarity between my own opinion and recording what the papers themselves say in a clear manner.
What did this study investigate?
This study looked at the use of puberty blockers in adolescent children under the age of 16. It measured their effect on feelings of gender dysphoria, as well as on general psychological well-being.
When and where did it take place?
Participants were recruited at the Amsterdam Gender Identity Clinic between 2000 – 2008 and the results were published in 2011. It is the first of two studies that looked at this same group of adolescents, and these are sometimes referred to together as the Dutch study or studies.
How did it work?
Participants were assessed using questionnaires, filled out at two separate times:
Shortly after first attending the clinic, before taking puberty blockers
After taking puberty blockers for some time, before continuing to any other treatment
These were completed by the patient themselves, parents and clinicians. The differences between the two sets of answers were used to assess the effects of the puberty blockers. On average, approximately 2 years elapsed between taking the two questionnaires.
Who was included?
To be eligible, adolescents would need to:
Be under 16 (those aged 16+ proceeded straight to cross-sex hormones)
Have persistently shown gender dysphoria since childhood
Live in a supportive environment
Have no serious psychiatric disorders that might interfere with assessment
e.g. the text highlights Autistic Spectrum Disorder as making this difficult
Have reached the initial stages of puberty (Tanner stage 2-3)
A total of 70 participants were selected, although not everyone completed all of the assessments.
What were the results?
The results section of the paper presents some detailed tables of data (see end) and highlights some specific observations.
Psychological Functioning
Child Behaviour Checklist (CBCL) and Youth Self-Report (YSR)
These questionnaires are completed by parents (CBCL) and the young person themselves (YSR) and assess a range of general behavioural and emotional problems. Some questions were excluded due to the fact they are not suited to children experiencing gender dysphoria.
A score of more than 63 is considered to indicate a clinical issue, with higher scores indicating a more significant effect on function. Three scores were recorded – separate ratings for “internalizing” and “externalizing” behaviours, as well as a total score.
Results of these questionnaires were available for 54 participants and the authors remark that there is a “significant decrease” in the average scores over the period of taking puberty blockers.

A similar pattern applies across each of the categories, representing an improvement in general behavioural and emotional problems.
In addition to the figures in the table, the authors provide information on the proportion of participants who scored in the clinical range, and noted a reduction after taking blockers:
Based on CBCL, this decreased from 44.4% to 22.2%
Based on YSR, this decreased from 29.6% to 11.1%
Beck Depression Inventory (BDI)
This is a multiple-choice questionnaire completed by the adolescent, and measures the level of depression on a numeric scale:
14 – 19: mild depression
20 – 28: moderate depression
29 or more: severe depression
Results of these questionnaires were available for 41 participants and, again, the authors note that these scores “significantly decreased” – i.e. depressive symptoms improved.

Trait Anger and Anxiety (TPI and STAI)
These are part of a larger set of tests (the Scales of the State-Trait Personality Inventory) and measure the tendency to respond with anxiety or anger to threatening or annoying situations. It presents 20 statements about how often these emotions are experienced and asks the adolescent to answer on a scale 1 (almost never) to 4 (almost always).
Results of these questionnaires were available for 41 participants and the authors remark that the scores showed no significant change.
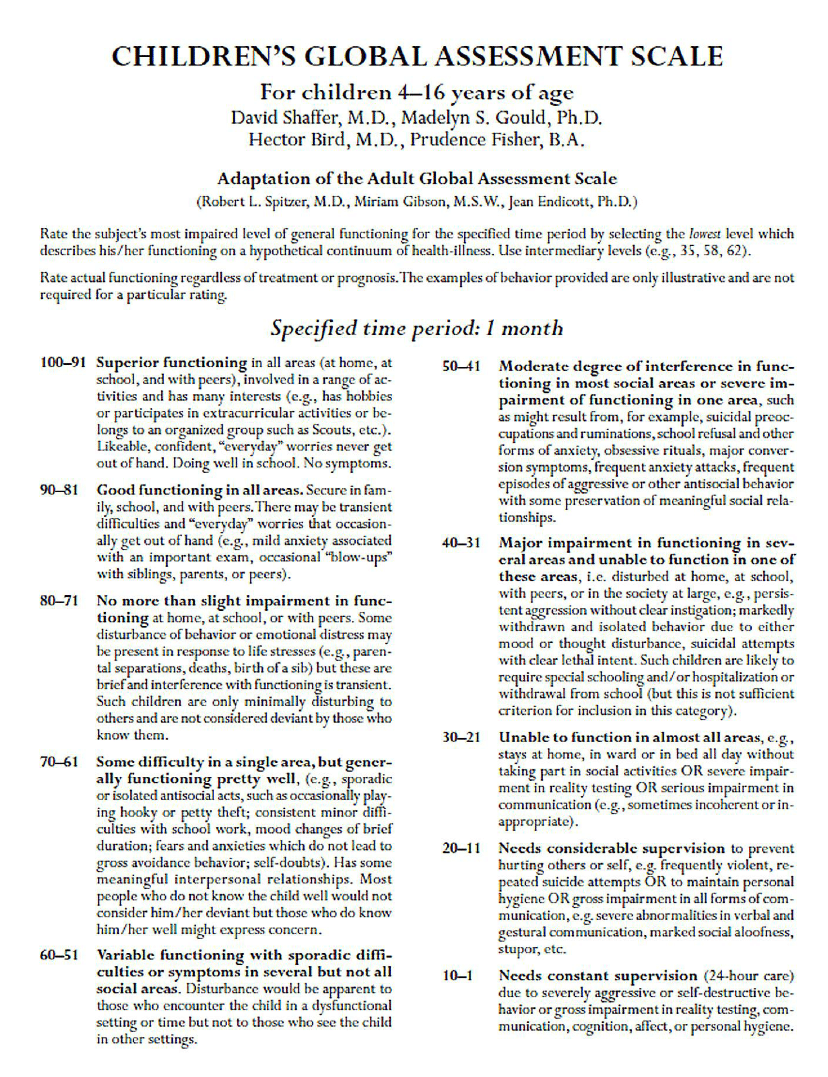
Children’s Global Assessment Scale (CGAS)
This is a general assessment of mental health in a child, with the clinician assessing impact on the patient’s ability to function in day-to-day life. A higher number indicates better global functioning or a lower level of disturbance. The scale is not stated in the paper itself, but I have sourced and included a copy in Appendix A, for reference.
Results of these questionnaires were available for 41 participants and the authors note that these scores “significantly increased” – i.e. function became less disturbed.

The relevant score ranges (taken from Appendix A) are:
71-80 No more than slight impairment in functioning
61-70 Some difficulty in a single area, but generally functioning pretty well
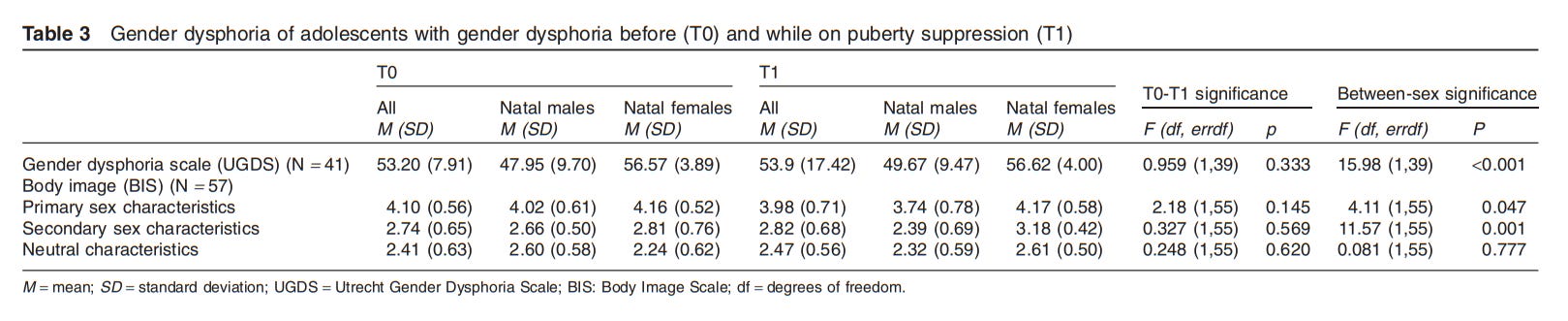
Gender Dysphoria
Utrecht Gender Dysphoria Scale (UGDS)
This was used to measure adolescents’ gender dysphoria. This takes the form of a set of statements and the young person rates their agreement on a 5-point scale. A higher score indicates greater dysphoria. The text gives an example statement of “I feel a continuous desire to be treated as a man/woman”.
Results of these questionnaires were available for 41 participants and the authors remark that, overall, their responses did not show any significant change in gender dysphoria.
Body Image Scale (BIS)
This asks the participant to rate 30 different body features on a 5-point scale, with a higher score indicating dissatisfaction. The results were grouped into three categories based on their relevance to gender: primary sex characteristics, secondary sex characteristics and neutral characteristics.
Results of these questionnaires were available for 57 participants and, again, the authors note that, overall, the responses did not indicate any significant change in gender dysphoria.
However, they do point out that an increase in scores was observed for females over the period taking blockers, indicating an increase in dysphoria. Conversely, this reduced for males over the period. (This meant that, when combined, there was minimal overall change.)

The authors also note that this measure indicates a higher level of dysphoria in biological females than in males both at the start and end of the studied period.
What else did the authors discuss?
Various potential reasons for the findings are suggested:
One possibility is that, because puberty blockers reduce changes to adolescents’ bodies, this means they retain an appearance that they feel fits better with their desired gender role. They note that, in adults, difficulty passing as the new gender is an issue that influences psychological problems (see reference 30) and thus imply the same may be true in this group.
Another idea offered is that because adolescents have been started on a treatment pathway, they feel reassured that further treatment will be offered if needed. This would reduce uncertainty and mean fewer worries over that possibility.
They remark that the effects of stigmatization and discrimination were likely to be limited, due to the exclusive selection of patients with a supportive environment around them.
They also note that participants were regularly seen by the clinic’s psychologists or psychiatrists, meaning any psychological problems could be addressed quickly, contributing to psychological well-being.
The point is made that the authors did not expect puberty blockers to resolve gender dysphoria – and lists other studies that point to cross-sex hormones and surgery being necessary for this (see references 7, 8, 32).
They note that none of the participants changed their mind about wishing to continue to further treatment whilst on puberty blockers.
They raise the fact that female participants in the study joined the study at a later age than males, meaning they tended to have progressed further through puberty, typically including breast development and beginning menstruation. A few theories are offered as to why they might seek help later:
Visible signs of puberty may be considered less dramatic in females than in males
Lower public awareness of treatment being available for females
Generally higher threshold for seeking clinical help in females
They also discuss some of the limitations of the study, including:
It does not consider the impact of social relationships or sexuality
It looks only at adolescents at an early stage of treatment, and longer term follow-up would be needed to establish whether the effects persist
It does not look at any physical effects of the puberty blockers, and notes this would be needed before any broad conclusions can be drawn about safety
They point out that ideally this would have been a blinded randomized controlled trial but note this is challenging to achieve. Reasons given are the difficulty in motivating adolescents to participate and possible ethical concerns over denying access to puberty suppression to those in the control group.
What did the authors conclude?
“Gender dysphoria did not resolve” as a result of taking puberty blockers
Psychological functioning “improved in various respects”
Statement made “cautiously” that puberty blockers “may be a valuable element” in managing adolescent gender dysphoria
Puberty blockers “[relieve] the acute distress accompanying gender dysphoria”
That they therefore “[help] in the exploration of suitable treatment options and making a balanced decision” regarding gender transition
Conflicts of interest
None were declared.
Full results tables
Please note: I do not own the rights to these images – they are taken from the paper itself. If you are one of the authors and would like me to take them down please get in touch.


References
The following list of references are cited by the study:
American Psychiatric Association. Diagnostic and statistical manual of mental disorders, DSM-IV-TR, 4th edition, text revision. Washington, DC: American Psychiatric Association; 2000. 2282 de Vries et al. J Sex Med 2011;8:2276–2283
World Health Organization. International statistical classification of diseases and related health problems. 10th edition. Geneva: World Health Organization; 1993.
Wallien MS, Cohen-Kettenis PT. Psychosexual outcome of gender-dysphoric children. J Am Acad Child Adolesc Psychiatry 2008;47:1413–23. 4
Zucker KJ, Bradley S. Gender identity disorder and psychosexual problems in children and adolescents. New York, NY: Guilford; 1995.
Cohen-Kettenis PT. Gender identity disorder in DSM? [letter]. J Am Acad Child Adolesc Psychiatry 2001;40:391.
Drummond KD, Bradley SJ, Peterson-Badali M, Zucker KJ. A follow-up study of girls with gender identity disorder. Dev Psychol 2008;44:34–45.
Cohen-Kettenis PT, van Goozen SH. Sex reassignment of adolescent transsexuals: A follow-up study. J Am Acad Child Adolesc Psychiatry 1997;36:263–71.
Smith YL, van Goozen SH, Cohen-Kettenis PT. Adolescents with gender identity disorder who were accepted or rejected for sex reassignment surgery: A prospective follow-up study. J Am Acad Child Adolesc Psychiatry 2001;40:472–81.
Cohen-Kettenis PT, van Goozen SH. Pubertal delay as an aid in diagnosis and treatment of a transsexual adolescent. Eur Child Adolesc Psychiatry 1998;7:246–8.
Shalev JE, Leung PC. Gonadotropin-releasing hormone and reproductive medicine. Obstet Gynaecol Can 2003;25:98–113.
Wren B. “I can accept my child is transsexual but if I ever see him in a dress I’ll hit him”: Dilemmas in parenting a transgendered adolescent. Clin Child Psychol Psychiatry Special Issue: Sexual identity and gender identity. 2002;7:377–97.
Grossman AH, D’Augelli AR. Transgender youth and lifethreatening behaviors. Suicide Life Threat Behav 2007;37: 527–37.
de Vries AL, Noens IL, Cohen-Kettenis PT, van BerckelaerOnnes IA, Doreleijers TA. Autism spectrum disorders in gender dysphoric children and adolescents. J Autism Dev Disord 2010 Jan 22 [Epub ahead of print] doi: 10.1007/s10803-010-0935-9.
Cohen-Kettenis PT, Delemarre-van de Waal HA, Gooren LJ. The treatment of adolescent transsexuals: Changing insights. J Sex Med 2008;5:1892–7.
Delemarre-van de Waal HA, Cohen-Kettenis PT. Clinical management of gender identity disorder in adolescents: A protocol on psychological and paediatric endocrinology aspects. Eur J Endocrinol 2006;155(suppl 1):S131–7.
Hembree WC, Cohen-Kettenis P, Delemarre-van de Waal HA, Gooren LJ, Meyer WJ, 3rd, Spack NP, Tangpricha V, Montori VM . Endocrine treatment of transsexual persons: An Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2009;94:3132–54.
Viner RM, Brain C, Carmichael P, Di Ceglie D. Sex on the brain: Dilemmas in the endocrine management of children and adolescents with gender identity disorder. Arch Dis Child 2005;90(suppl II):A78.
WISC-R Project group. Wechsler Intelligence Scale for Children-Revised (WISC-R), Dutch version. Lisse: Swets and Zeitlinger; 1986.
Wechsler D, Kort W, Compaan EL, Bleichrodt N, Resing WCM, Schittkatte M. Wechsler Intelligence Scale for Children—Third Edition (WISC-III). 3rd edition. Lisse: Swets and Zettlinger; 2002.
Wechsler D. Wechsler Adult Intelligence Scale—Third edition (WAIS-III), Dutch version. 3rd edition. Lisse: Swets and Zetlinger; 1997.
Verhulst FC, van der Ende J, Koot HM. Handleiding voor de Youth Self Report (Manual for the Youth Self Report). Rotterdam: Department of Child and Adolescent Psychiatry, Erasmus University; 1997.
Verhulst FC, van der Ende J, Koot HM. Handleiding voor de CBCL 4–18 (Manual for the Child Behavior Checklist and Revised Child Behavior Profile). Rotterdam: Department of Child and Adolescent Psychiatry, Erasmus University; 1996.
Cohen-Kettenis PT, Owen A, Kaijser VG, Bradley SJ, Zucker KJ. Demographic characteristics, social competence, and behavior problems in children with gender identity disorder: A cross-national, cross-clinic comparative analysis. J Abnorm Child Psychol 2003;31:41–53.
24. van der Does AJW. BDI-II-NL. Manual for the Dutch version of the Beck Depression Inventory. 2nd edition. Lisse: Harcourt Test Publishers; 2002.
25. van der Ploeg HM. Handleiding bij de Zelf Beoordelings Vragenlijst (Manual of the Dutch version of the Spielberger Trait Anxiety Inventory, STAI-DY). 2nd edition. Lisse: Swets Test Publishers; 2000.
Van der Ploeg HM, Defares PB, Spielberger CD. Dutch version of the Spielberger State-Trait Anger Scale. Lisse: Swets and Zeitlinger; 1982.
Shaffer D, Fisher P, Lucas CP, Dulcan MK, Schwab-Stone ME. A children’s global assessment scale (CGAS). Arch Gen Psychiatry 1983;40:1228–31.
Lindgren TW, Pauly IB. A body image scale for evaluating transsexuals. Arch Sex Behav 1975;4:639–56.
Kuiper AJ. Transsexualiteit: Evaluatie van de Geslachtsaanpassende Behandeling. Amsterdam: Free University Press; 1991.
Ross MW, Need JA. Effects of adequacy of gender reassignment surgery on psychological adjustment: A follow-up of fourteen male-to-female patients. Arch Sex Behav 1989;18: 145–53.
Savin-Williams RC, Ream GL. Suicide attempts among sexual-minority male youth. J Clin Child Adolesc Psychol 2003;32:509–22.
Murad MH, Elamin MB, Garcia MZ, Mullan RJ, Murad A, Erwin PJ, Montori VM. Hormonal therapy and sex reassignment: A systematic review and meta-analysis of quality of life and psychosocial outcomes. Clin Endocrinol (Oxf) 2009.
Giordano S. Lives in a chiaroscuro. Should we suspend the puberty of children with gender identity disorder? J Med Ethics 2008;34:580–4.
Appendix A – CGAS Ratings
The original paper defining this scale is available here:
https://pubmed.ncbi.nlm.nih.gov/6639293/
As this is not available without a fee, I have used a copy that was reproduced here:
https://www.researchgate.net/publication/272824387_On_the_Children's_Global_Assessment_Scale
When looking up scientific papers online, you may often find you only have access to the abstract, but you can usually have some luck finding the full paper online by googling something like “full text” along with the full name of the paper.
TERRIFIC idea.
Start with a "Why Is This Study Important To Parents?" section.
You did great with the translation you did. It's still way too long and technical. Parents just need the basics, the BASIC basics. I suggest that your goal be to use the same language you would use explaining it to your neighbor while chatting over your backyard fence, or chatting before or after a meeting with someone. Casual, straightforward, plain language.
Leave out the numbers and charts. Too technical. And also overblown. This is fancy dressing up of a silly multiple-choice questionnaire, only a little bit more detailed than the questionnaire people fill out about their health every time they go to the doctor.
Keep It Simple and Short. Use bullet points.
Add "What Do Trans Activists Claim That This Proves?" section and a "Why Does It Not Prove That At All?" sections.